Han B.-C., "The burnout society". Stanford Briefs, 2015. Cover by 4eyesdesign
a manifesto on (neuro)endocrinology
Introduction
Here we present a practical, non-marketable therapy for hair loss. The observations presented here are the fruit of self-examination and rely on a hypothetical etiology, that constitutes the core contribution, since the therapy — a specific type of massage — originates its rationale developing from others' work on endothelial thinning[7C, Ustener E. et al, 8L] and dysbiosis; indeed, one of the first result of massaging may be draining sebum rather than revascularization.
Results are commented here, here and here for open discussion.
The concept of “tanning and thinning” as central balding factors is key to this exploration. It challenges the apparent opposition between sclerotization (hardening) and thinning. In reality, hardened material can easily look “deflated.” Dry, fibrotic tissue loses elasticity and, unlike a hydrated or living medium, can’t maintain cohesive volume. In this light, sclerotization reflects not reinforcement but loss of veicular function — and thinning becomes the consequent loss of regenerative potential.
Keep this in mind as who's writing emphasises on this false friend and it gets to mean closure, not even thinning! But in general, a process of hardening should always pop up as a gateway to paralysis, hardness and strength are death’s companions. So as a little gloss:
Sclerotization: loss of fluidification or increase in tension.
Thinning: degrowth in biological tissue.
Thickness: swelling of tissue not prone to loss of elasticity.
The report proposes a vascular–mechanical etiology for androgenetic alopecia (AGA as an umbrella condition), emphasizing endothelial motility loss and tissue stress as contributors to AR sensitivity and regenerative collapse. Based on self-observation and cross-domain evidence, we present "scalp over skull" massage as a non-pharmacological intervention capable of restoring perfusion, elasticity, and signaling readiness.
Rather than developing a new therapy, we reinterpret an old one—massage—through this lens. The technique, focused on "scalp over skull" motion, is grounded in observed effects on drainage and tissue softness.
Various non-pharmacological practices are already tested and recognized as effective in the real world, but the paradigm shift toward a purely non-medical approach is constructed and justified across this piece by extended references to different medical subfields, along with our philosophical take from Byung-Chul Han's The burnout society, which will constitute the sole direct quotations in the main text, for readability.
Quotes outside of the enumeration come from closed or introductive sources.
Your author has only heard of Illich's Medical Nemesis and is only halfway through another critic of medical history, M. Van Der Meensche's Bodies and Souls, but the profession of the latter writer helps you understand our critical take: disease and solutions that may be deemed trivial, like strictly cosmetic surgery or hygiene in sensible places, underlie sometime-subjective vicious circles that the world is faster to cut at the symptom than to cure at the source. Emphasis on premature palliative care reflects the "positivation of the world [that] allows new forms of violence to emerge. They do not stem from the immunologically Other. Rather, they are immanent in the system itself" and reasonate with it. Epidemics of the reason may as well be treated as social or normative problems.
Our recall of current etiologies and presentation of an alternative aims at pinpointing the largest demographics that may benefit from a simple, "pro bono" method.
* [()]
*
Dimension and methods
This report is based on self-experimentation, with observations thus far limited to a single subject (the author). To approach generalizability, intersecting cross-demographic factors will be considered here. We depart from conventional etiologies of hair loss[8I], which typically emphasize primarly follicular pathology. Vascular involvement is discussed in literature as perifollicular inflammation or ischemia, and a foundational reclassification is attempted.
In this work, a “vertical” differentiation is proposed: alopecia may be interpreted as a form of endothelial deficiency (mechanical), rather than a disorder of the follicle. Supporting this, neurogenic skin inflammation has been shown to inhibit hair growth[3B]; male androgenetic alopecia is associated with increased arterial stiffness[4A]; and angiogenesis is required for normal follicle development in animal models[4E]. Dermatitis is a highly prevalent condition, with some analyses suggesting its global disease burden may approach that of chronic disorders such as diabetes[3E] (so all dermal layers are involved).
A second vertical perspective centers on the role of tissue hormonal stress over metabolic oscillations or genetic deficiencies. The hypothalamic-pituitary-adrenal axis (HPA), as well as prolactin and catecholamines, are acknowledged as principal stress mediators, and stress is widely recognized as a major aggravating factor in hair loss[3B]. Hair follicles serve as a useful model for studying neuroendocrine-immune interactions in the context of stress.
Conventional treatments — such as minoxidil and finasteride — appear to function via vasodilatory and androgen-suppressing effects, reinforcing the importance of vascular and hormonal context[4A].
Scalp massage is reported to improve hair thickness and cutaneous softness by enhancing local blood flow, and mechanical forces such as stretching may influence gene expression relevant to hair and skin health[3D]. If such forces were shown to improve both relaxation in tissue and circulating signals, we would have a model parallel to the current pharmacological interventions.
A third vertical axis considers the functional role of hair in human biology, especially in thermoregulation[3C] and specialized sensory input[9D], with homeostatic stress system activity considered essential to follicular health[Chrousos G. P.]. Not circulatory support to the scalp, or hormonal distress from homeostasis whereas the centrality itself of the follicle and its holistic function as stress mediator. Stress-induced hyperactivity evidence would reinforce the relaxation pathway we envision and a connection between hair and general health is remarkably found in correlation with cardiovascular health (CVH)[4B].
That would confirm general health urgency. The tendency to treat hair loss solely as a cosmetic concern may thus obscure underlying systemic dynamics [3C].
These three verticals form a vascular triad model of sclerotization, cardiovascular burden and flow capacity: respectively mechanical, circulatory and sensorial shock.
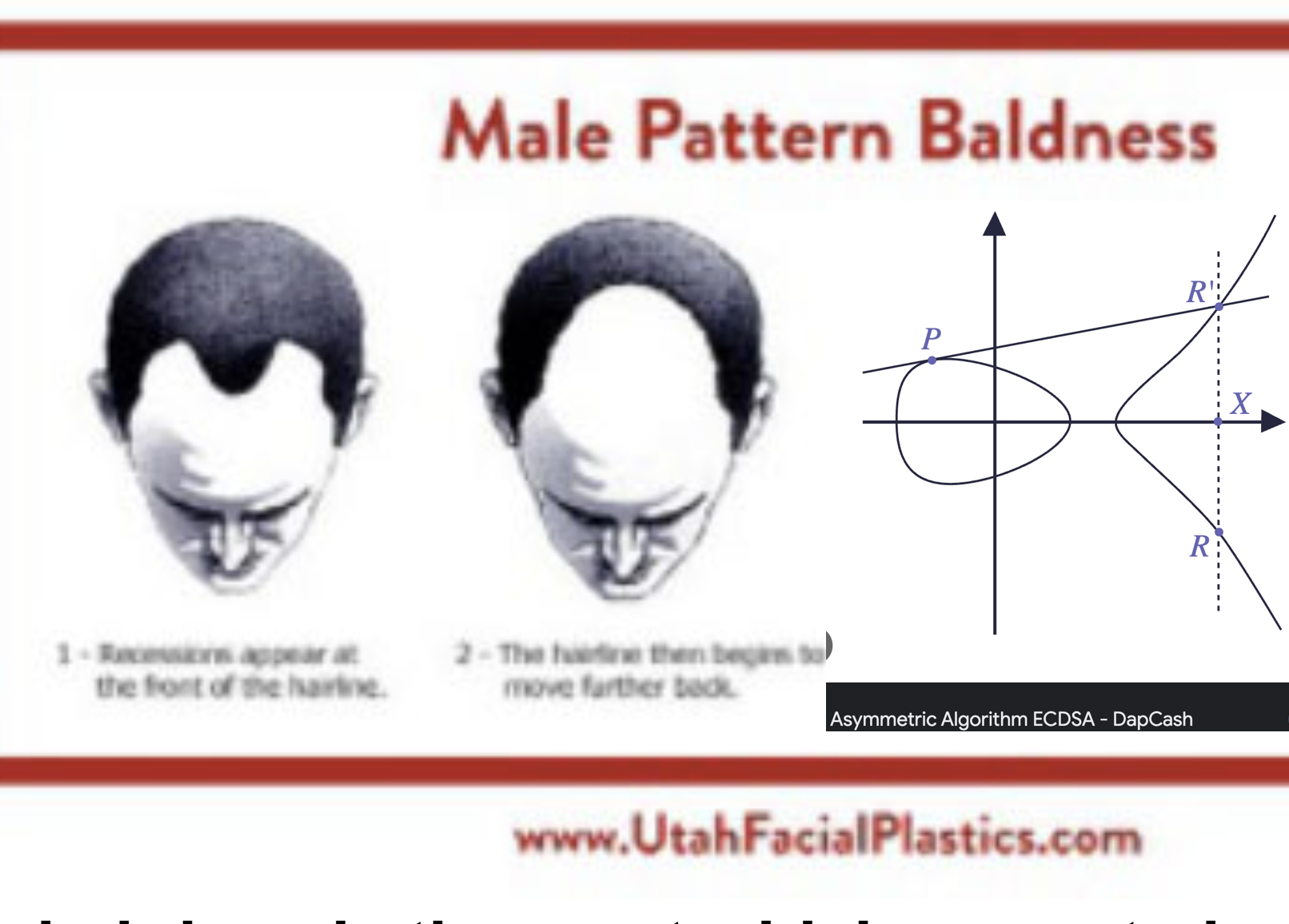
The prevalence of hair loss among men is striking, as fewer than 15% escape some degree of baldness by the age of 70[4A]. In addition to treatments targeting specific pathways, such as testosterone modulation (Finasteride, Dutasteride), lifestyle and environmental factors—such as sleep quality[3C, 6C] or pollutants oxydation[8L] (and oxydative stress in general[7F] )—have been recognized as modifiable contributors, particularly when intervention occurs early in the disease course.
Notably, detachment of the arrector pili muscle predicts irreversible loss, underlining the importance of early intervention.
Building on the earlier “stress” vertical, a further horizontal dimension is psychosomatic: the psychological and neurogenic aspects of hair loss are increasingly recognized. This perspective aligns with emerging psychotrichology, where hair serves as a model for understanding the physiological effects of stress[3B]. Even the challenge of reliably reproducing in vivo experimental results in hair research may be related to profound neuroimmunological effects of environmental stressors.
The evolutionary context of eso-socially patterned baldness[9D] adds to hair’s hormonal sensitivity, with follicles functioning both as hormone targets and as localized sources of hormones[3B], as a "cosmetic" signal that goes beyond 'aesthetics'—indeed, sensation and self-manifestation of deeper states of health.
In the present work, we acknowledge these psychosomatic and sociological axes as possible co-factors. Baldness and boldness as an antinomy[Florenskij P.A.] may serve a clue into the sociosomatic deference of skin issues.
But we need to focus on objective, biological demographics, isolating two upstream, quantifiable features—follicular anchoring (FA) and androgen receptor (AR) sensitivity—as primary filters distinguishing populations most prone to androgenetic alopecia (AGA).
Other environmental, social, inflammatory, and mechanical factors are thus best conceptualized as co-factors: they may accelerate or amplify AGA in individuals with the underlying demographic susceptibility (i.e., weak FA and/or heightened AR).
Essential Logic: AGA Susceptibility Across Populations
Now for a brief exception to our readability-friendly quote policy:
A) Caucasians tend to lose more hair
“Caucasians tend to lose the most hair. Additionally, West Asian (specifically Indian) people are likely to experience similar hair loss levels to Caucasians – followed by Afro-Caribbean people.
The hair loss statistics of the Hispanic community are difficult to determine.”[8B]
B) Africans have stronger follicular anchoring (FA) than Caucasians
“Most black patients tend to have thicker dermal tissue in their scalp.” [8C]
“Previous studies suggest that the increased compact stratum corneum and thicker dermal sheaths with better-aligned collagen fibers and more abundant ground substances in African-descended patients contribute to increased resistance to FUE punches.” [8D]
“Finally, other studies have suggested that there is a greater lipid content in black stratum corneum compared with white stratum corneum. This could account for the greater density of black stratum corneum, a conclusion supported by Weigand et al.” [8E]
C) Caucasians exhibit intermediate androgen levels—higher than East Asians, lower than Sub-Saharan Africans
“Differential-K theory proposes that levels of androgen… differ across three large racial groups with Sub-Saharan Africans having the highest levels, East Asians the lowest, and Caucasians… being intermediate.”
“East Asians showed signs of the lowest androgen level for most indicators and were lower than Caucasians on all of them.” [Dutton E. et al]
D) FA × AR explains A
Caucasians are most AGA-prone because they combine (relatively) less robust follicular anchoring (B) with (relatively) higher androgen/AR sensitivity (C), resulting in the highest rates of hair loss (A).
Upstream Mapping
Androgen receptor signaling mediates miniaturization but is shaped by both genetic factors (AR gene variants) and environmental cues (stress, inflammation). Mechanical interventions (e.g., massage) have shown potential to influence the extracellular matrix (ECM) and local AR signaling [3D].
Accordingly, for early- and moderate-stage AGA, system-level, non-invasive interventions could be prioritized as exploratory therapy, while reserving pharmacological strategies for cases where follicular-level dysregulation persists despite upstream correction.
Factor
Disease Mechanism
Population Impact
Addressed by Pharmacology?
Addressed by Massage?
Intervention Logic
Androgen Receptor (AR) Overload / DHT
DHT binds to AR, triggering follicular miniaturization and hair cycle shortening. [8F, 8G]
Primary driver in genetically susceptible males; frequency and severity highest in populations with high AR activity. (Shorter Cytosine-Adenine-Guanine repeats, DHT sensitivity)
Yes (finasteride, dutasteride) [5H, 8H, 8K]
Indirect (massage may modulate AR via mechanotransduction and stress reduction)
Pharma targets hormonal pathway; massage potentially co-modulates AR via tissue tension [3D]
FA thinning / ECM Sclerotization
ECM breakdown, reduced stem cell support, loss of follicle stability, increased tissue stiffness and loss of elasticity. Aging and chronic microtrauma diminishing dermal thickness and subcutaneous cushioning. [8F, Ustener E. et al]
More severe and earlier in Western populations due to demographic FA vulnerability. Aging and chronic stress exacerbate loss of elasticity and anchoring
Minoxidil partial (short-term vasodilation, keratinocyte proliferation to some extent [1F, 4K]) Fin/Dut may reverse DHT-induced skin thinning [8F]. "Hyperresponders" may indeed have this happening over time. (see .5 for pyroptosis and extreme dryness)
Yes (improves ECM pliability, microcirculation, and elasticity)
Massage restores elasticity and supports follicular architecture, counteracting sclerotization and anchoring loss
Vascular-Inflammatory Burden
Endothelial dysfunction, reduced scalp blood flow, and chronic inflammation create a feed-forward loop of follicular hypoxia, cytokine elevation, oxidative damage and fibrosis. [4I, Ustener E. et al, 4J, 3F, 3G]
Worsens with age, stress, comorbidities, and urban environmental load (see .3)
Baldness can be viewed as a manifestation of systemic circulatory-orthostatic failure, not merely local follicular degeneration. Vascular insufficiency—or “dryness” defined as lack of nutrient flow—undermines follicular health.
The body’s reliance on water and adequate perfusion is fundamental both for solution levels and chemo-electrical conducitivty. Hair follicles are metabolically active[6E] and require consistent vascular support. The epicranial aponeurosis is a dense, fibrous layer with limited intrinsic vascularity, and with aging, dermal capillary rarefaction and ECM stiffening reduce perfusion in the subgaleal and dermal zones[4A, Ustener E. et al, 4L, 4M], plausibly contributing to AGA.
Physiological environments—particularly during tissue regeneration—are inherently dynamic, with ongoing extracellular matrix remodeling that modulates cell behavior and gene expression. This dynamic quality is evident in emerging biomaterial research, where scaffolds responsive to external stimuli (such as magnetic fields) can achieve large-scale stiffness changes, promoting stem cell differentiation while maintaining biocompatibility[1A, 1B].
In the scalp context, this suggests that interventions capable of dynamically modulating tissue stiffness—such as massage—may restore the mechanical and vascular environment necessary for follicular health, counteracting the sclerotic remodeling observed in AGA; not only that, but modulating stress, helping corticotropins support keratinocyte survival and barrier function.
Keratinocytes help prevent water loss, and lighter skins (as in the demographics shown) may be more vulnerable to such loss due to both keratinocyte irresponsiveness and sun sensitivity (cfr. “pyroptosis”[3F]). [3A, 4A, 4K]
An interesting set-back, or deeper step to take, would be consideration of black and white lipid content. DHT may suppress melanin synthesis[8E, 8F].
Regions with high vascularity and metabolic activity—such as facial, axillary, and pubic areas—retain elastic connective tissue and robust hair growth, in contrast to the scalp and forehead. Androgens stimulate growth in these zones, while scalp follicles under AGA may suppress growth factors.
* [()]
*
.1 – Stress, Cleansing, and Endothelial Burden
The skin expresses local cortisol signaling pathways, mirroring the central HPA axis and functioning as a stress sensor[3A]. Scalp fascia is dense in mechanoreceptors[9A], and hair follicles contribute to sensory adaptation through mechanotransduction pathways[9C, 9D].
Local cortisol and mechanosensory inputs translate psychosocial and thermal fluctuations into biological effects on hair cycling. Vasomotor tone modulates heat exchange and local metabolic load, linking vascular tone to the scalp’s ability to dissipate or retain heat [2B].
Acute stress narrows perifollicular capillaries in murine models, demonstrating a neurovascular stress response[3A]. Reducing muscle tension is routinely recommended to support scalp perfusion[3C]. Sleep-driven lymphatic and waste clearance, while less studied in the scalp, likely supports tissue homeostasis[2A]. Migraine models show meningeal inflammation, lymphatic output, and pain are linked, reinforcing a fluid-based contribution[3B, 6A].
Stress-driven increases in cortisol elevate transepidermal water loss, weakening the skin barrier and increasing vulnerability to dermatoses[3B]. It's plausible that barrier dysfunction and perfusion loss form a reinforcing cycle whose direction may trigger degeneration or reaction.
Physiological adaptation to heat—via environmental exposure or exertion—increases water loss, highlighting a tradeoff between thermal adaptation and hydration status[2B].
This dynamic may converge, imposing cumulative endothelial burden and progressive decline in the scalp structure and pipes. Machinic routine "is kerygmatic. [It] embodies 'pure being without any predicate.'" Levees break. "Tiredness has a broad heart". Cells retreat on themselves and set an alarm - DHT indeed stimulates hair grow. But "private tiredness, not ours, but mine over here and yours over there" exhausts communication and "proves violent because it destroys all that is common or shared, all proximity, and even language itself".
*
[()]
**
.2 – Pains of a Boiling Frog
Chronic pain may serve as the body’s metabolic detection of low perfusion or lymphatic stagnation—particularly through fascial nociception and neuroimmune amplification.
The psychosomatic overlap of pain is robustly documented in psychodermatology, showing that pain is entangled with emotional and cognitive states. Psychological stress further impairs the skin barrier by downregulating antimicrobial peptides and increasing vulnerability to infection in animal models[3A, 4A].
Fascial tissues, by virtue of their load-bearing function and dense innervation, are susceptible to nociceptive signaling under excessive tension or microtearing[7B]. Yet these signals can be twisted constructively as with microneedling. "A small amount of self-inflicted harm [Gewalt] protects one from a much larger danger, which would prove deadly". But lacking space for receiving or processing such signals, empty, open spaces of negative pressure - leads to self-referential build up. "Because Otherness is disappearing, we live in a time that is poor in negativity. [As in the story of Pierino e il lupo, today,] generalized communication and surplus information threaten to overwhelm all human defenses."
Perfusion failure disrupts the follicular cycle and balance, leading to reduced density and thickness, mediated by cytokines and angiogenic factors[3C]. Circulatory stress contributes to follicular dysfunction[4A, 4E]. The skin’s androgen metabolism links vascular compromise and pain[4A]. As follicles become more hypoxic, local androgen metabolism may drive pain and degeneration and chronic tissue stress can amplify pain signaling. Senescent neurons, including both directly injured and bystander cells, are a major source of IL-6, a key SASP cytokine implicated in nociceptor hyperexcitability.
"Even Nietzsche, who replaced Being with Will, knew that human life ends in deadly hyperactivity when every contemplative [beschaulich] element is driven out".
Targeted elimination of senescent cells in nerve-injured mice resulted in improved nociceptive behaviors, suggesting that cellular senescence is a modifiable driver of persistent pain[6B].
Tissue that stays active remains active — like neurons fire and wire — from "a pathological standpoint, the incipient twenty-first century is determined neither by bacteria nor by viruses, but by neurons"; on the other hand, sclerotizazion and follicular miniaturization in the scalp are associated with diminished regenerative potential [3C, 4A, 4E]. Dampened metabolism may result in fats deposit[7D]. Restoring microcirculation may work both downstream and upstream of current pharmacological interventions, respectively restoring flow capacity as obtained with vasodilation by Minoxidil and silencing androgenic stress like Finasteride/Dutasteride.
If hair acted as a terrain subclinical health signal (a "metabolic echo")[5C], and tissues maintain homeostasis through secretion of cytokines, growth factors, and peptides[9A], contributing to their activity and clearance through progressive stimulation (and deathrophization through activation) of the scalp should have a profound impact on the biome. Interventions like low-level light therapy (LLLT) and microneedling promote growth factor release, stem cell activation, and angiogenesis, suggesting a feedback loop between sensory input and metabolic response.
* [()]
*
.3 – Posture
Chronic cervical muscle tension impairs blood flow, irritates nerves, and slows the movement of fluids through skin and connective tissue.
Long-term strain narrows capillaries and disrupts scalp autonomic regulation. Fascia and connective tissue distribute tension throughout the cranial–cervical axis; when chronically stiffened, these networks lose elasticity, impeding fluid exchange and sensor coordination. Structures like Piezo1 channels—mechanical force sensors found in various tissues—illustrate the emerging recognition that tension-bearing matrices shape physiological signaling[9C]. Their role in scalp dynamics remains underexplored, but their presence reflects a wider principle: mechanical stress, if unresolved, can desynchronize the structural–neural interface.
Cervical spine misalignment or forward head posture can stretch and compress nerves and blood vessels, impairing systems, from breathing and digestion to circulation. These distortions increase sleep apnea risk and destabilize vital rhythms[7A, 7F].
Postural habits are thus influencing regeneration and maintenance throughout the body.
Animals, lacking homes, are conserving fur and the highest degree of motility. For humans with sedentariety came disconnection, atomization, overlooking "the systemic violence inhabiting achievement society, which provokes psychic infarctions. It is not the imperative only to belong to oneself, but the pressure to achieve that causes exhaustive depression. See in this light, burnout syndrome does not express the exhausted self so much as the exhausted, burnt-out soul." With Faust I made a mistake... it was a colossal, memorable mistake... That wretch had no soul at all, and for this reason he seemed to overflow with it: he was possessed only by an inextinguishable frenzy of planning, of continuous doing and undoing, with no other purpose than the action itself. (F. Savater, Creature dell'aria). You don't need a face to connect, just electricity, let alone hair. We're undergoing the same marbling process of wagyu calves - we're becoming statues. "The general denarrativization of the world is reinforcing the feeling of fleetingness. It makes life bare."
We're not protected from the sun anymore. "Now bare, sheer life itself is holy, and so it must be preserved at any cost." External social cues like hair are sacrifiable in principle when we're well oiled part of urbanization. Accomodating for such life style welcomes higher hormonal excursion when moving is needed. While overtraining is counterproductive, and complete sedentariety leads to death, the basal state of testosterone much like basal temperature are indexes of health. A dysregulation between the former and androgen cycles - as in hair cycle - should be investigated, considering that castrated males don't lose hair. Androgen excursion may explain the "paradox" of DHT both promoting vellus into beard and correlating with hair loss[8L].
“Dermal depressive failure” names the skin’s inability to maintain balance under prolonged chemical or vascular stress—a breakdown that mirrors postural or metabolic decline. Posing barriers, saying no doesn't work - the "violence of positivity does not deprive, it saturates; it does not exclude, it exhausts. That is why it proves inaccessible to unmediated perception." Hair as a metabolic echo persist like an inconvenient witness. "The late-modern achievement-subject, with a surplus of options at its disposal, proves incapable of intensive bonding. Depression severs all attachments."
Poor posture is widespread and often left uncorrected, leaving regions like the scalp underperfused [7A]. Mental and physical stress reinforce this, interrupting feedback loops that regulate vascular tone and thermal balance [3B].
The modern “head-down” life—bureaucratic, screen-bound—mirrors the cultural indifference (of men) toward male hair loss: too late, unprompt, looking for a one-shot or a little, five-seconds pill. Prevention, self-care, prohibitions, "commandements, and the law are replaced by projects, initiatives, and motivation." Harassing others to conceive status is the other side of the coin, subjugating facial tension to this passive-aggressive mechanism [9G, cfr. Florenskij P.A.]. "The exploiter is simultaneously the exploited[,] who exploits itself as his own vassal." "The capitalist economy absolutizes survival. It is not concerned with the good life. [...] It takes livingness from life [...] stripped of all trascendent value [the] inner logic of achievement society dictates its evolution into a doping society." "Health becomes self-referential".
*
[()]
**
.4 – Stimulation
The cure shall be "eloquent, seeing, reconciliatory tiredness in opposition to speechless, sightless, divisive tiredness. [...] One sees, and one is seen. One touches, and one is touched. [...] I am not tired 'of you' [...] but rather [...] 'with you'." Suppressing stress hormones is very different than downregulating their peak. Letting circulation flow means not only bringing nutrients to the hair and clearing their waste products - it also means signaling to the body that unprompt levels of DHT are being produced, precisely there.
Both glabrous and hairy skin are mechanosensory organs, but respond differently[9D].
Hair operates as a sensory interface, integrating thermal, hormonal, and mechanical inputs. Mechanosensory neurons respond to hair movement, pressure, and touch[9D, 3B].
Though humans lack vibrissae, the scalp and periauricular areas retain sensory functions, follicles are embedded neurovascular units.
Mast cells release nitric oxide, cytokines, and VEGF—key in vascular and inflammatory responses[3B]. Platelets and megakaryocytes, produced in bone marrow and regulated by lung signals, influence vascular dynamics[4D]. Wound healing capacity is a core tissue function [1C, 1E, 5I]. Postural strain and fascial stiffness reduce skin pliability and disrupt oxygenation, breaking loops essential to follicle health. Hair loss is not just a symptom but a regulatory element in this system, at the forefront of the skin barrier.
Loss of such functions hints at subtle changes in the organism that plausibly go undetected to the subject longer than they go to hair.
Hair loss may signal failed dissipative control over inflammation. Recovery requires mobilizing the regenerative capacity of organs[9C, 9A].
Interventions target this system: minoxidil boosts blood flow[3C]; massage and microneedling restore elasticity; capsaicin may enhance neurovascular tone; androgen blockers reduce sebum production by lowering DHT, potentially altering the scalp’s evaporative dynamics and thermal buffering. Fascia underpins all of these systems[9A].
But how does Minoxidil address vascular thickening? Does vasodilation prioritize vascular density?
* [()]
*
.5 – Stimulation as Signal-Restoration
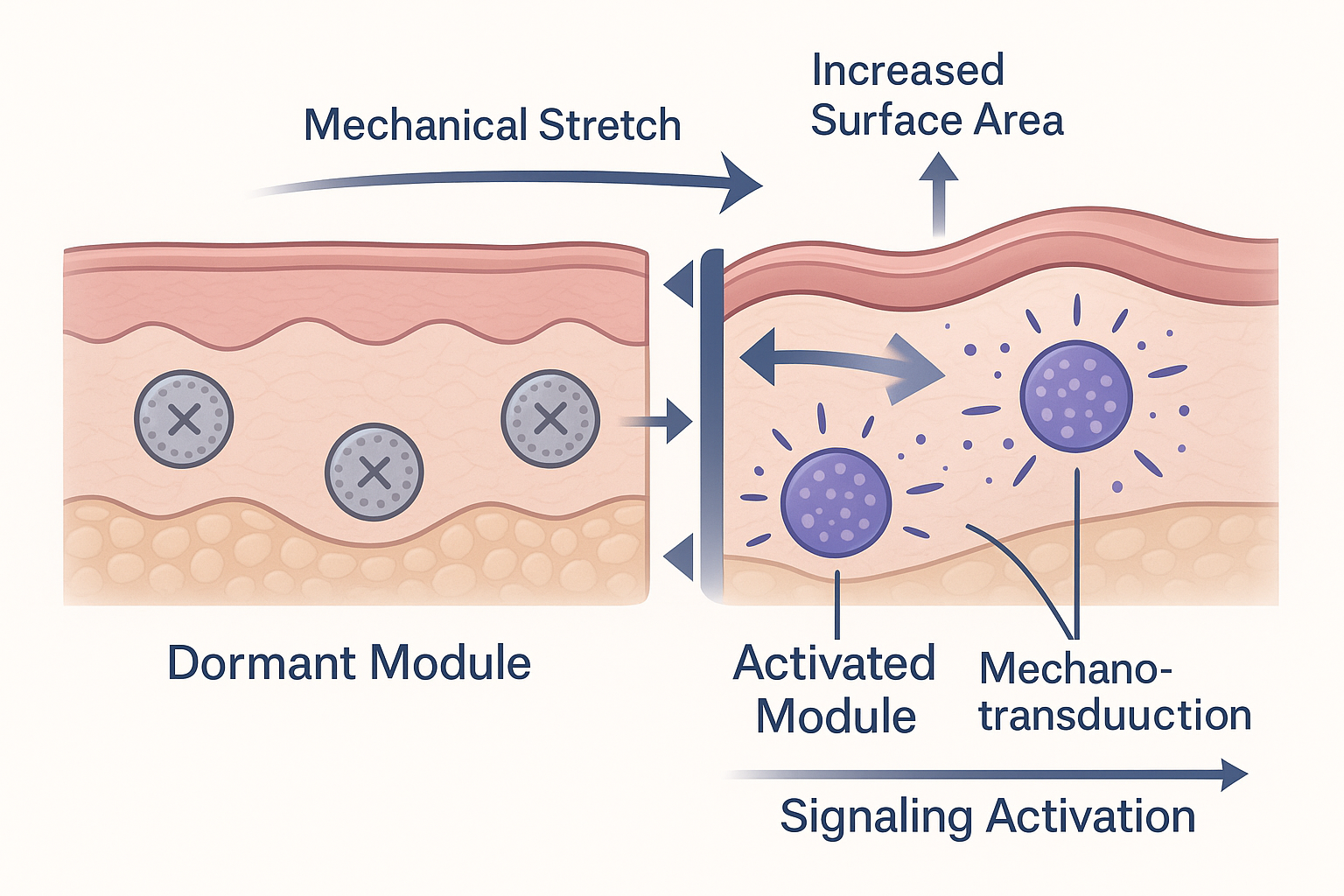
By inducing vascular density instead of vasodilation, sensory surface increases. Indeed taking the brain as an analogy, its jagged surface is a feature to extend it. Wider surface area may also help dissipating heat. thankyou ChatGPT and Perplexity
Massage, when applied with sufficient pressure and rhythm, acts as a targeted mechanical signal to subdermal and fascial tissues[3C]. In the context of fascial collapse (see .3), it restores interstitial and perineural signaling by reintroducing gradient forces—pressure, shear, and stretch—which activate mechanotransduction cascades[9A, 7B]. These inputs trigger viscoelastic remodeling (creep, relaxation, mild microtearing), reducing stiffness and restoring a regenerative environment.
DHT is converted from other androgens in peripheral tissues[5K]. It's also involved in the growth of prostate. Male reproductive features are external per se: fertilizing agents reach for an outside-in incubator.
Cold exposure in relationship with the arrector pili (see Dimensions and methods, on detachment and irreversible loss from it) is being investigated[6F]. Piloerection, or horripilation, happens from cold, but also from electricity. If the scalp fascia was effectively a tensile transmitter, continuation of the elastic skin on the neck that protects from whiplash, sense of temperature and mechanotransduction would come together under the umbrella of recent work on piezo channels[9H]. It's impossible to tackle such a complex, evolutionary relationship between different sensations in the restricted context of scalp health - who is the chicken, inflammation, who is the egg, stress?
The easiest thing to do would be considering the simple physical law that PV = nRT. Like vascular density, sensory surface and heat dissipation due to biological exhaustion (overgrown biotissue needs increased metabolism and so depletes energy from the rest of an organism) cohexist, still a system that strives for homeostasis has to keep up with such physical limitation[Musk E.]. If there is a limit to sufferable vascular pressure, than the only way to increase heat resistance is by volume. Minoxidil does this with vasodilation. But if DHT is to offer increased tissue resistance to burn (DHT is shown to help heal burn wounds[3H]), such tissue would represent higher quality material for biological heat resistance than blood.
Excess DHT may provoke tissue into outflowing and not surviving detached from its biological home - but healthy DHT levels may be key to increase actual density of regulators in the same volume.
If overproduction of DHT was due to inflammation, a reclassification of this problem as autoimmune may be successful. Keratinocytes and DHT seem to be regulating the process by which skin protects the body from solar insult[3F, 3H]. "Self-absorption does not produce gratification, it produces injury to the self; erasing the line between self and other means that nothing new, nothing 'other,' ever enters the self [...]. Self-love means taking an explicit stand vis-à-vis the Other. Narcissism, in contrast, blurs the border. If one suffers from a narcissistic disorder, one sinks into oneself." One cannot gaze at the sun, not immersed in oneself with eye closed, not without ground support.
"Learning to see means 'getting your eyes used to calm, to patience, to letting things come to you' [...]. Reacting immediately, yielding to every impulse, already amounts to illness and represents a symptom of exhaustion".
Accomodating for a sensory-friendly cellular substrate by reducing its stiffness is achievable through massage, and further goals of hydration and bulging are at hand.
This mechanical signaling can also increase oxytocin and lower vasopressin in craniofacial regions[9B], modulate systemic hormones via circulation and shift autonomic tone—particularly through osteopathic techniques[9A].
By stimulating dermal–follicular units both mechanically and neurologically, manual therapy can affect local inflammation, sebum levels, and broader neural circuits. Stress peptides modulate immunity, pigmentation, and antimicrobial defenses in skin[3A]. These signals are transduced through barrier-resident cells like keratinocytes and melanocytes, linking local and systemic responses[5E, 4K, 8J].
Treating the skin as a signaling filter between the internal biome and external ports helps sustain vitality at the interface between cellular homeostasis and environmental turbulence. Techniques like breathing, massage, and relaxation help re-establish balance between internal physiology and environmental load.
*
[()]
**
the guts came back
.6 – Characterising Sensory Tissue
Sensory function in the craniofacial and scalp region arises from layered networks of mechanoreceptors, fascia-integrated structures, and afferent nerves, which together convert touch, pressure, and tension into systemic signaling[9C].
The scalp and facial skin contain Merkel cells and Pacinian corpuscles for detecting pressure and vibration[9D], along with C-tactile afferents (affective touch) and Ruffini endings (shear/stretch). The fascial network—periosteal, endomysial, and perimysial layers—acts as the body’s largest sensory and proprioceptive organ[7B].
The superficial fascia (galea aponeurotica)[7F] distributes mechanical loads across cranial compartments. Fascial fibroblasts express Piezo1 channels, potentially influencing both glial and vascular systems[9C].
The skin responds to mechanical input such as massage or low-level light therapy by modulating oxytocin, cortisol, and immune activity[9B]. This sensory interface likely helps regulate stem cell activation and stress resilience.
Follicular regeneration, in contrast to muscle hypertrophy, depends on coordinated vascular, metabolic, and immune conditions—rather than mechanical loading[3C].
Fascia operates as a dynamic signaling matrix. Biotensegrity models frame it as a structural filter that interprets mechanical and environmental signals at scale[7B].
These considerations do not imply therapeutic certainty but frame a broader exploration: what does it mean that sensory tissues organize regeneration? "The vita contemplativa is not a matter of passive affirmation and being open to whatever happens. Instead, it offers resistance to crowding, intrusive stimuli. Instead of surrendering the gaze to external impulses, it steers them in sovereign fashion."
In what quality different parts of the scalp differ in sensory features? mechanical loads are discussed for AGA patterns[Ustener E. et al] but adding the thermoregulative dimension address a basal charachteristic of human: forehead is bald. This vertical zone underneath the horizontal sheat that's constantly exposed to the sun is bald as the rear neck in a specular fashion. It's also non flexible, unlike the nape, so the main skull-protection it provides is in being a homogeneous protuberance. A very flat protuberance that can accumulate a lot of pus and lose hair starting from the zones furthest from the rest of hairless face. Indeed, two indentations are formed between long-lasting, side hair and hair over the nose. As if breathing, and the cooling effect that comes with it, was particularly functional for the forehead.
A conclusive speculation is that different sensory tissue features different apparatus, turning pathology-target co-factors faceted. Sensory tissues organize regeneration in that they react to different needs from different areas of the body. In this view, scalp massage is not symptomatic care but a way of engaging the upstream dynamics of tissue logic, potentially reactivating processes suppressed in numbness. Unlike muscle hypertrophy coming from mechanical load, the load such tissues bear, and the activity they're justified to metabolise, is sensory.
* [()]
*
.7 – (re)generation
The skin, as the body’s largest organ, functions as a barrier to environmental stressors and supports the matrix necessary for follicular regeneration[5A].
Scalp hair likely evolved to reduce solar absorption and conserve sweat, especially in early bipedal hominins in arid climates. Tightly curled hair minimizes heat gain and moisture loss, optimizing cerebral cooling[5A, 5B].
With evolution new sources of inflammation come and mental burden - viral "violence cannot account for neuronal illnesses such as depression, ADHD, or burnout syndrome, for it follows the immunological scheme of inside and outside. [...] Burnout syndrome occurs when the ego overheats, which follows from too much of the Same." Too much of hair promotion from DHT - it's useless. But it's possible that moving it around, making it circulate from a vexed follicle to those around...
Adequate oxygenation is critical[9G]. The lungs contribute to tissue repair by producing platelets and PDGF[4D]. Hypoxia accelerates cellular senescence and hinders follicular recovery. DHT has been seen operating as both tissue healing promoter and delayer [3H]. Cortisol and androgens effectively cause hirsutism.
Hair co-evolution as thermoregulator and social cue while losing the external barriers it poses in wild ecosystem exposes a loss of function in motility feedback. Loss of touch, "social" (environmental) stress and severed mobility from the animal state - flying, fitting in balls like water, being "multi-tasking" - when conflict still "founds personal identity" - diminishes the need for external metabolism driven by sensory curiosity. "What proves problematic is not individual competition per se, but rather its self-referentiality, which escalates into absolute competition", at complete loss of openness - the "late-modern achievemnt-subject [...] liberates itself into a project." One day I will grow back, says the recessive follicle while suffocating with DHT.
While DHT helps with the creation of reproductive organs and modulates other vescicles in wound healing, these aren't cronic processes. Hair have long reproductive cycles - 3, 4 years - and this makes it possible to reverse and prevent long term degneration - but it's also a sacrifiable process in this intricate economy of endocrine modulators.
Hair cycling depends on precise environmental conditions: oxygenation, temperature, vascular tone, and tissue flexibility all influence whether follicles remain dormant or re-enter growth. While certain immune and adipose cell types appear to trigger the early regenerative phase—by releasing repair signals or responding to cold stimuli—these effects likely converge within mechanical and metabolic readiness[5A, 9C].
Rather than focusing on isolated pathways, it's suggested that regeneration emerges when upstream constraints—hypoxia, stiffness, thermal stress—are lifted. Massage and other sensory interventions may achieve this by reactivating tissue communication networks and restoring baseline conditions for growth.
These insights expand regeneration from a cell-level event to a condition that emerges from systemic readiness. If follicles depend on oxygen, elasticity, and metabolic exchange, then interventions that restore those properties deserve closer scrutiny. [Peña O. I. G., Zavala M. A. L., Ruelas H. C.]
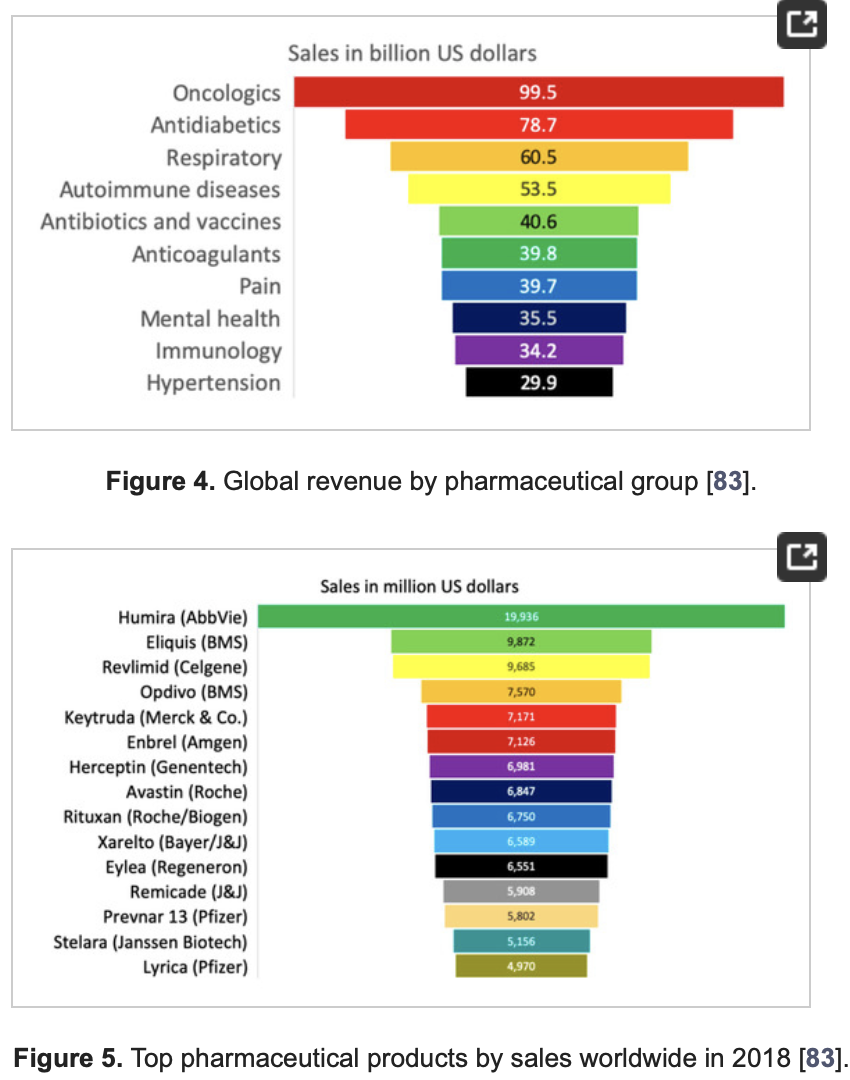
It may be significant that the state of the market is akin to the situation in the anticoagulant sector, without results - aside from costly patches; a relatively minor segment (6th biggest in the world) with a single drug (Eliquis, 9.9B revenue) that is second biggest after an anti-inflammatory (Humira, 20B).
Was hair loss condition clearer in its etiology, current pharma wouldn't feel like a shot in the dark. It's significant of a market considered aesthetic — but, if we were right, rooting in a severe condition such as vascular injury.
Massage reconditions this terrain—consolidating circulation, softening fascia, activating sensory feedback—where pharmacology does not. Environmental and behavioral factors—hydration, thermal stress, microcirculation—modulate this regenerative potential, making the restoration of tissue “readiness” (vitality, potential) a prerequisite for effective therapy.
True regeneration re-emerges only when upstream readiness—vascular, metabolic, sensory—is restored[4J]. At that point, both FA and AR act within a recovered landscape.
*
[()]
**
Conclusions and Limitations
Our (me and the Lost in the Norwoods army) work built a complex etiology around a condition that would raise more awareness given a different context: for example, if our pets were to lose their fur, we'd be worried with all such of serious illnesses up to autoimmune disease (or cytokine storms as seen in COVID and other hypotheses such as scalp atrophy in sclerosis[3F, 2C])—a path already suggested for Alopecia Areata[5J]. This etiology tries to cover and conserve what's already considered working—vasodilation for Minoxidil, androgens homeostasis for Finasteride—and expand on it: respectively, vasodilation isn't the same as complex angiogenesis, and hormones should be treated as signals, not symptoms. With a twist, perpetrator "and victim can no longer be distinguished."
ahah just being sketchy here ... ...unless
In particular, the vascular triad model (cardiovascular burden, sclerotization, and flow capacity) offers a focused angle that recontextualizes AGA severity as not merely genetic or hormonal but circulatory in its chronicity. This proposal, while anchored in mechanistic plausibility and supported by cross-domain comorbid correlations, lacks direct longitudinal testing.
As mentioned in the Dimensions section, the aspects of scalp composition, thickness, and density may be a prompt for more differential analysis.
Alopecia is better read as a surface expression of systemic conditions, adaptive energetics, and sociosomatics—not only follicular failure... "self-refentiality produces a paradoxical freedom that [...manifest...] psychic indisposition" to cure. Care time is neglected! The burden remains to not reduce this complexity prematurely but to stage our research questions carefully, in tune with the multidimensionality of the problem.
One emerging speculative question is whether skeletal morphology (such as cranial bone structure) modulates vascular behavior or mechanical stress across scalp zones.
Because the cervical spine integrates autonomic regulation, its mechanical dysfunction can extend scalp hypoperfusion into broader systemic instability.
An unresolved axis may exist between cranial morphology and skin plasticity, particularly in the calcification-prone zones where perfusion loss accelerates.
We propose competition between bones and skin in stem homeostasis[9E, Ustener E. et al, 1C, 1D, 4J, 7F]. Does bone density and large shape make for thicker skin? We see plants as a model where cortical and ciliary tissues have found balance.
There's no evolutionary reason (ontological, except thermoregulation[5B]) for going bald, except maybe "looking" more aggressive, masculine, and even having some hedge in combat, as the hair usually remaining, if grasped, gets your opponent's hand closer to teeth, which one could use as a weapon. Is this a relic of testosterone related aggressiveness?[5C].
We see a strong evolutionary rationale (gnoseological) for going bald as a signal of underlying conditions: CVH, dehydration, which if untreated are way worse than any psychological distress; signaling to conscience to rest is a good feature. "C[o]lture presumes an environment in which deep attention is possible."
Given all of this, we're on theoretical ground, with close to no evidence, and would like to contribute to an exploratory prompt.
Alcohol and smoke as good options
A shout-out to our sponsors.
It's known that alcohol helps nutrients reach deeper tissues (A. Schwarzeneger on alcohol) and that nicotine is a vasodilator (more ambiguously than niacin).
We hope for a future with safe-consumption options of these products.
Florenskij, P. A., "La colonna e il fondamento della verità. Saggio di teodicea in 12 lettere"
Dutton E. et al, "Population differences in androgen levels: A test of the Differential K theory". PaID, 2016
Musk E., physics are the law, everything else is recommendation, twitter, twitter.
Peña O. I. G., Zavala M. A. L., Ruelas H. C., "Pharmaceuticals Market, Consumption Trends and Disease Incidence Are Not Driving the Pharmaceutical Research on Water and Wastewater." ERPH, 2021
Ustener E. et al, "Cause of Androgenic Alopecia: Crux of the Matter". PRS, 2013
1 Tissues and Biomimetics:
1A Li, J. et al, "Magnetic Liquid Metal Scaffold with Dynamically Tunable Stiffness for Bone Tissue Engineering". Bioactive Materials, 2022
1B Bertagnolli, R., "Paving the way to more precise tissue engineering with help from metal". Linkedin
1C Barnes, M., "The Role of Blood Flow in Reversing Hair Loss". Cellustrious, 2023
3D Koyama T. et al, "Scalp massage and dermal papilla cells". PMC, 2016
3E Peter M., "Itching is a stress factor". medizinonline, 2022
3F Sawaya M., "Inflammation in androgenetic alopecia". ISHRS, 2012
3G Slominski, A., Zmijewski M., "Glucocorticoids inhibit wound healing". JID, 2017
3H Shi H. et al, "Controlled dual release of dihydrotestosterone and flutamide from polycaprolactone electrospun scaffolds accelerate burn wound healing". FASEB, 2022
4 Vascular Health & Perfusion:
4A Asfour L. et al, "Male Androgenetic Alopecia". Endotext, 2023
4B Thom et al., "Metabolic Syndrome, Cardiovascular Disease and the Hair Growth Cycle: Addressing hair growth disruptions using Nourkrin® with Marilex® as a proteoglycan replacement therapy: A concise review" dermatojournal, 2018
4D Lefrançais E. et al., “The lung is a site of platelet biogenesis and a reservoir for hematopoietic progenitors.” Nature , 2017
4E Yano, K. et al., "Control of hair growth and follicle size by VEGF-mediated angiogenesis". JCI, 2001
4I Kato H. et al, "The Effects of Ischemia and Hyperoxygenation on Hair Growth and Cycle". Organogenesis, 2020
4J Zhou S. et al, "Crosstalk between endothelial cells and dermal papilla entails hair regeneration and angiogenesis during aging". JAR, 2025
4K Stamatas G. N. et al, "Minoxidil topical foam in men with androgenetic alopecia: signaling pathway analysis". Cell Cycle, 2017
4L Jin K. et al, "A Microcirculatory Theory of Aging". Aging & Disease, 2019
4M Bentov I., Reed M. J., "The effect of aging on the cutaneous microvasculature". Microvascular Research, 2019
5 Sensorial and Hormonal Pathways:
5A Park S., "Hair Follicle Morphogenesis During Embryogenesis, Neogenesis, and Organogenesis". Cell Dev Biol, 2022
5B Lasisi T. et al, "Human scalp hair as a thermoregulatory adaptation". PNAS, 2023
5C Sapolsky R., "Testosterone doesn't make you aggressive..." YouTube
5D Tanimura S. et al, "Hair Follicle Stem Cells Provide a Functional Niche for Melanocyte Stem Cells". Cell Stem Cell, 2011
5E Kiso M. et al, "Sox21 disruption causes cyclic alopecia in mice". PNAS, 2009
5I Lu C. et al, "PRP-derived exosomes stimulate hair follicle growth via Wnt/β-Catenin". Regenerative Therapy, 2025
5J Burma N. E., Ramien M. L., "Cutaneous and Gut Dysbiosis in Alopecia Areata". JID Innovations, 2025
5K Antoniou-Tsigkos A., "Adrenal Androgens". Endotext, 2019
6 Neural Pain & Terrain Signaling:
6A Nelson-Maney N. P. et al, "Meningeal lymphatic CGRP signaling and migraine". JCI, 2024
6B Kim D. et al, "Aging and injury drive neuronal senescence in the dorsal root ganglia". Nat Neurosci, 2025
6C Kinoshita F. L. et al, "Synaptic dynamics during the sleep–wake cycle". PLOS Biology, 2025
6E Meng H., "Trace Elements and Atherosclerosis Diagnosis". RCM, 2023
6F "Physio-metabolic method of treating androgenic alopecia. Cold receptors. The relationship between DHT, cold receptors, minoxidil and antiandrogens.". discussion on Reddit, 2024
7 Fascial & Vascular Compression:
7A Hauser R., "Forward head posture symptoms and complications". Caring Medical
7B Schleip R. et al, "The fascial network and pain". 7th IWC, 2010
7C Lin L. et al, "High-frequency ultrasonography of the scalp in AGA". SR&T, 2024
7D Tabataiei M. R. et al, "Sonographic comparison of subcutaneous fat layer thickness in the scalp area in patients with androgenetic alopecia compared to healthy individuals: Cross-sectional". SR&T, 2024
7F Sadgrove N. J. et al, "The 'bald' phenotype and western diet". TFS&T, 2021
8 Demographics & AR Pathways:
8B Dubey S., "Ethnicity And Hair Loss Patterns". Austin Hair Clinic, 2022
8C UGraft, "Hair Transplants for African American Patients". UGraft, 2021
8D Sanusi U. et al, "FUE in African Descent: A Skin-Responsive Technique". Dermatologic Surgery, 2023
8E Taylor S. C., "Skin of color: biology, structure, implications". JAAD, 2002
8F Fu D. et al, "DHT-induced hair regrowth inhibition via AR activation". Biomed Pharmacother, 2021
8G Li K. et al, "AR/miR-221/IGF-1 pathway in AGA". Int J Biol Sci, 2023
8H Hatanaka T. et al, "Gene expression in follicles: dutasteride and finasteride". SMJ, 2022
8I Lin Y. S. et al, "Multidisciplinary approach to hair treatment". Exp Dermatol, 2019
8J Li J. et al, "Gsdma3 required for follicle differentiation in mice". B&B RC, 2010
8K Kaufman K. D. et al., "Finasteride in treatment of AGA". JAAD, 1998
8L Williams R. et al., "Getting under the skin of hair aging: the impact of the hair follicle environment". Experimental Dermatology, 2020
9 Mechanotransduction & Massage Physiology:
9A Bordoni B., Escher A., "Fascial Manual Medicine: The Concept of Fascial Continuum". Cureus, 2025
9B Morhenn V. et al, "Massage increases oxytocin and reduces ACTH". PubMed, 2012
9C Pathak M. M. et al, "Piezo1 channels in neural stem cells". PNAS, 2014
9D Abraira V. E., Ginty D. D., "Sensory neurons of touch". Neuron, 2013
9E Gaunitz W. E., "On calcification". YouTube, 2024
9F Wang J. et al, "PIEZO1-mediated signaling in follicle stem cells". Cell Biol, 2025
9G "Hair Loss: Are The Real Underlying Causes Androgenetic?" TMD - occlusion
9H "Discoveries of receptors for temperature and touch" Nobelforsamlingen, 2021
 Keratinocytes help prevent water loss, and lighter skins (as in the demographics shown) may be more vulnerable to such loss due to both keratinocyte irresponsiveness and sun sensitivity (cfr. “pyroptosis”
Keratinocytes help prevent water loss, and lighter skins (as in the demographics shown) may be more vulnerable to such loss due to both keratinocyte irresponsiveness and sun sensitivity (cfr. “pyroptosis” The skin expresses local cortisol signaling pathways, mirroring the central HPA axis and functioning as a stress sensor
The skin expresses local cortisol signaling pathways, mirroring the central HPA axis and functioning as a stress sensor